Recognizing and Working with Client Dysregulation: Quick Tips for Therapists


Think of the nervous system as the system that tells all the other systems what to do. It oversees our survival by orchestrating our body’s response to the world into fluid but discrete autonomic states. These states play a big part in shaping how we think, feel, and interact with others.
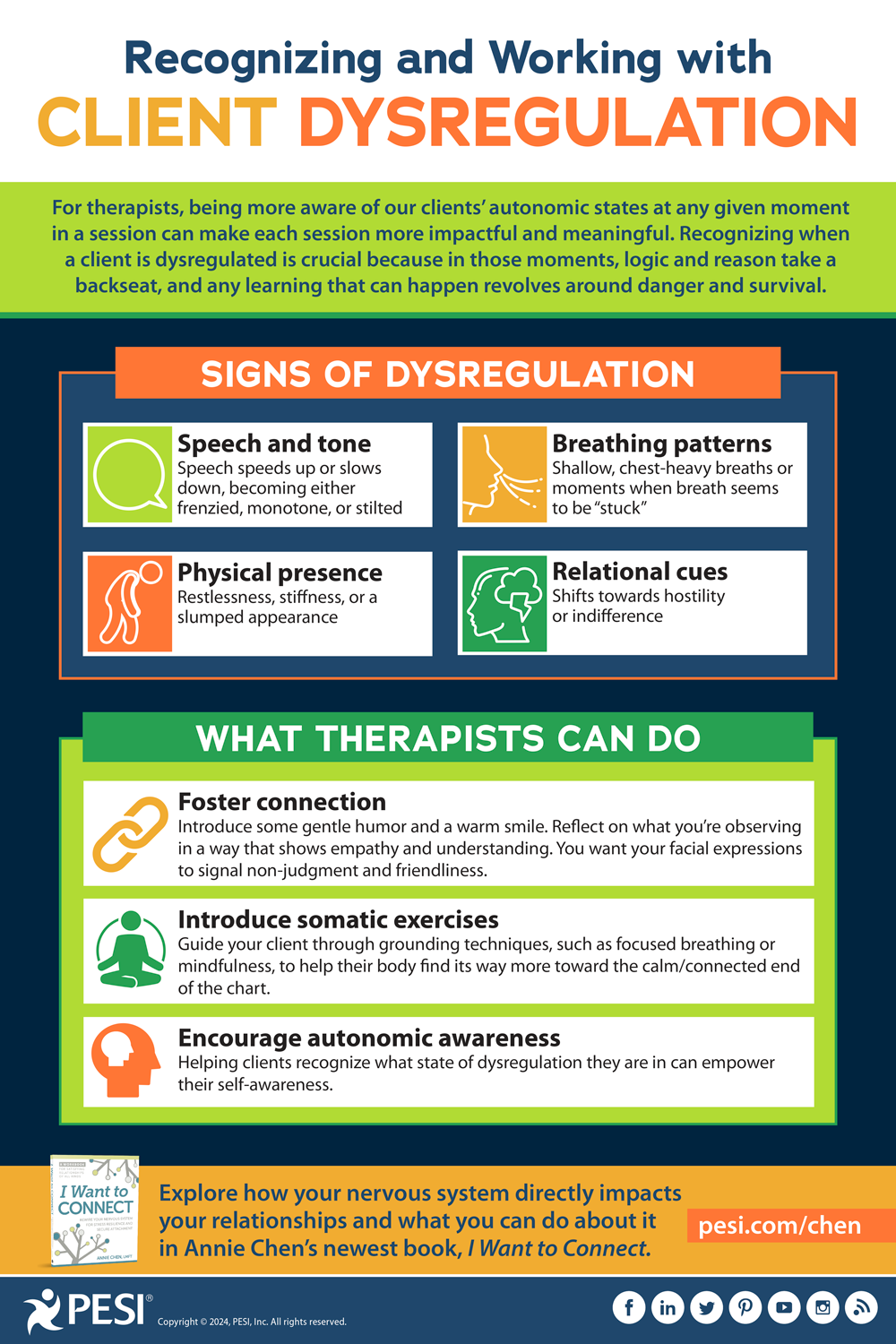
For therapists, being more aware of our clients’ autonomic states at any given moment in a session can make each session more impactful and meaningful.
In my latest book, I Want to Connect: Rewire Your Nervous System for Stress Resilience and Secure Attachment, I unveil a chart that demystifies what this would look like, offering a polyvagal-informed map to identify and understand dysregulation. This tool is designed to simplify the complexity of our nervous system’s responses, providing clients and therapists with a clear roadmap for understanding dysregulation.

For more explanation of these states, including how to recognize each one, check out Demystifying Dysregulation: Navigating Your Autonomic States.
Why does this matter? Recognizing when a client is dysregulated is crucial because in those moments, logic and reason take a backseat, and any learning that can happen revolves around danger and survival. Here are the telltale signs of dysregulation to watch for:
For therapists, being more aware of our clients’ autonomic states at any given moment in a session can make each session more impactful and meaningful.
In my latest book, I Want to Connect: Rewire Your Nervous System for Stress Resilience and Secure Attachment, I unveil a chart that demystifies what this would look like, offering a polyvagal-informed map to identify and understand dysregulation. This tool is designed to simplify the complexity of our nervous system’s responses, providing clients and therapists with a clear roadmap for understanding dysregulation.
For more explanation of these states, including how to recognize each one, check out Demystifying Dysregulation: Navigating Your Autonomic States.
Why does this matter? Recognizing when a client is dysregulated is crucial because in those moments, logic and reason take a backseat, and any learning that can happen revolves around danger and survival. Here are the telltale signs of dysregulation to watch for:
- Speech and tone: Speech speeds up or slows down, becoming either frenzied, monotone, or stilted
- Physical presence: Restlessness, stiffness, or a slumped appearance
- Breathing patterns: Shallow, chest-heavy breaths or moments when breath seems to be “stuck”
- Relational cues: Shifts towards hostility or indifference
- Foster connection: Introduce some gentle humor and a warm smile. Reflect on what you’re observing in a way that shows empathy and understanding. You want your facial expressions to signal non-judgment and friendliness.
- Introduce somatic exercises: Guide your client through grounding techniques, such as focused breathing or mindfulness, to help their body find its way more toward the calm/connected end of the chart.
- Encourage autonomic awareness: Helping clients recognize what state of dysregulation they are in can empower their self-awareness.
Rewire Your Nervous System for Stress Resilience and Secure Attachment

In I Want to Connect, a follow-up to the popular The Attachment Theory Workbook, expert relationship therapist Annie Chen explores how your nervous system directly impacts your relationships and what you can do about it. Weaving together insights from Polyvagal Theory, somatic practices, and relationship co-regulation skills, this workbook addresses a range of issues through a central connecting point: that the state of our nervous system either primes us for resilience and connection or pushes us toward defense and shutdown.
Online Course:
Integrating Attachment Science to Maximize Treatment with IFS, EFIT, Polyvagal Theory, EMDR and More
Integrating Attachment Science to Maximize Treatment with IFS, EFIT, Polyvagal Theory, EMDR and More

Revolutionize your practice through the power of attachment! This online training brings together leading experts in attachment science, including Dan Siegel, Dan Hughes, Claire Mellenthin and many others. Discover today's most popular, evidence-based approaches in psychotherapy - Emotionally Focused Individual Therapy (EFIT), Internal Family Systems (IFS), Expressive Therapies, and more – so you can help clients of all ages loosen the grip of attachment ruptures, restore sense of self, and develop the ability to connect and repair.
You May Also Be Interested In These Related Blog Posts



